
Simple, evidence-based ways to boost milk supply: nursing and pumping schedules, power pumping, latch help, paced bottle feeding, hydration, galactagogues, a...
Exclusive Pumping: Schedules, Supply, and Weaning
Sarah Mitchell
Sarah Mitchell is a Registered Pediatric Nurse and a mother of three who has spent over a decade helping families navigate the beautiful, chaotic early years of childhood. She combines evidence-based medical knowledge with real-world parenting experience to offer practical, compassionate advice. At Awesome Parent, Sarah's mission is to help exhausted parents find solutions, trust their instincts, and finally get some sleep.
Exclusive pumping is breastfeeding, just with extra dishes. If you are here because latching has been a struggle, baby is in the NICU, you are heading back to work, or you simply prefer the predictability of bottles, you are not doing it “wrong.” You are feeding your baby and that counts.
Below is a realistic roadmap: how to set up a pump routine that protects your supply, sample schedules by age, flange fit basics, quick troubleshooting, storage guidelines, and how to wean without turning your chest into a science experiment gone rogue.
If you only read one thing: In the first weeks, milk removal is the job. Aim for frequent, comfortable sessions with a flange that fits, and fix pump parts before you blame your body.

How it works
Milk production runs on demand and removal. Your body pays attention to how often milk is removed and how thoroughly the breasts are emptied. In the early weeks, frequent, effective pumping helps establish “production capacity.” Later, once supply is more stable, many parents can pump less often and still meet baby’s needs.
If you have ever heard about “cluster feeding,” exclusive pumping has a similar concept. Instead of baby doing the clustering, you create frequent removal with the pump, especially in the first 2 to 6 weeks.
Two practical goals to keep in mind:
- Total pumps per day and total milk removed matter more than perfect timing.
- Comfort and consistency beat heroic, painful pumping sessions every time.
Getting set up
Pick a pump that matches your goals
If you are exclusively pumping, a reliable double electric pump is usually the workhorse. Wearable pumps can be helpful, but some people find they do not empty as well as a traditional setup, especially early on. If your supply feels fragile, start with the strongest, most efficient option you can access, then add convenience tools later. The test is output and comfort, not the marketing.
If baby is in the NICU
If your baby is premature or hospitalized, ask your team about using a hospital-grade pump and pumping as soon as you can after delivery (often within the first few hours when possible). Skin-to-skin care, when allowed, can also help. Follow NICU guidance first, always.
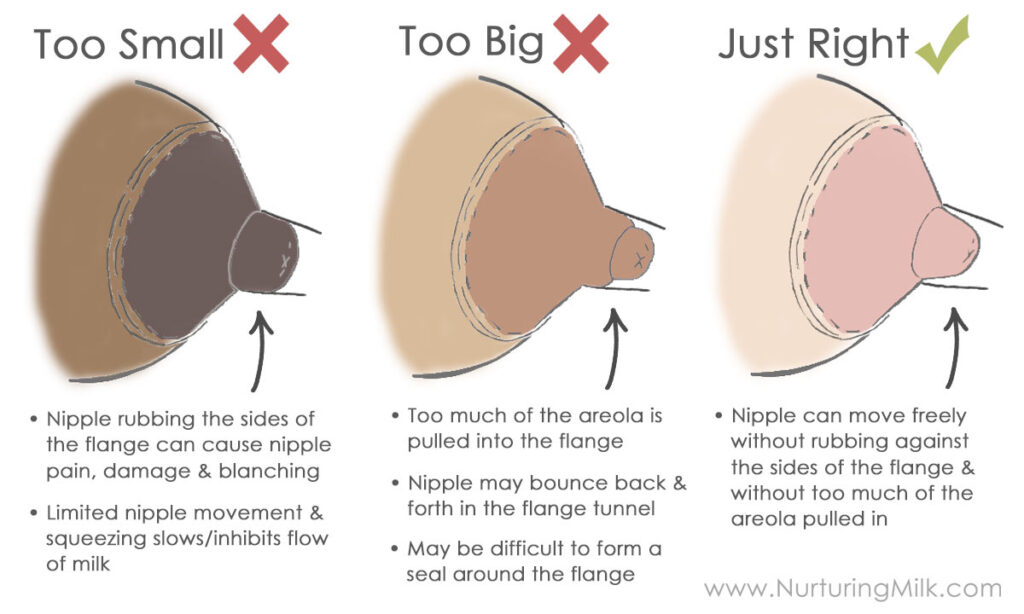
Flange fit matters more than most people realize
In clinical settings, I saw plenty of “low supply” stories that were actually “wrong flange size plus pain.” A good flange fit helps you empty better and protects your nipples.
- What you want: nipple moves freely in the tunnel, minimal areola pulled in, and pumping should feel like strong tugging, not sharp pain.
- Too small: rubbing, pinching, a white ring at the base of the nipple, or blisters.
- Too large: lots of areola pulled in, swelling, and you feel like you need higher suction to get milk out.
How to measure: Measure your nipple (not areola) before pumping or when it is not swollen, then add a small amount of extra room, often about 1 to 3 mm, depending on the flange brand. Re-check if you have swelling, pain, or a sudden output change.
How often to pump
These are starting points, not moral rules. Some parents need more sessions to build supply. Others can do fewer and still meet baby’s needs. If your baby was premature, had a tough start, or you are trying to increase supply, lean toward the higher frequency.
Birth to 2 weeks
- Aim for: 8 to 12 pumping sessions per 24 hours
- Spacing: about every 2 to 3 hours, with one slightly longer stretch at night if you can
- Session length: 15 to 20 minutes, or 2 to 5 minutes after milk slows to drops
2 to 6 weeks
- Aim for: 7 to 10 sessions per 24 hours
- Tip: keep at least one overnight pump if your supply is still building
- Session length: 15 to 25 minutes depending on flow and letdowns
6 to 12 weeks
- Aim for: 6 to 8 sessions per 24 hours
- Common pattern: every 3 hours during the day, plus one overnight or very early morning pump
3 to 6 months
- Aim for: 5 to 7 sessions per 24 hours
- Note: many parents keep the early morning pump because output is often highest then
6+ months (while continuing breast milk)
- Aim for: 4 to 6 sessions per 24 hours, adjusted for solids and your goals
- Reality check: some babies still take the same milk volume even after starting solids
Example day (newborn)
6am, 8:30am, 11am, 1:30pm, 4pm, 6:30pm, 9pm, 11:30pm, 2am, 4am
Example day (3 to 6 months)
6am, 9:30am, 1pm, 4:30pm, 8pm, 11pm
How long to pump per session
“Empty” is not a single moment. It is more like: strong flow, then slowing, then another letdown, then drops. Many people do best with 2 letdowns per session. A practical target:
- Early weeks: 15 to 20 minutes, or a few minutes after milk slows to drops
- Established supply: often 15 to 25 minutes, depending on your letdowns
- If you are still spraying at 30 minutes: you might need a different flange size, settings, or more frequent sessions instead of just longer sessions
If you are also bottle-feeding pumped milk, consider using paced bottle-feeding techniques so baby can control the flow and take what they need without guzzling. That can reduce spit-up and help your supply match baby’s true appetite.
How much milk is typical
Milk needs vary a lot. Instead of chasing a single magic number, focus on trends, diapers, and weight gain with your pediatrician. A few helpful benchmarks:
- Early days: colostrum amounts are tiny. Milliliters matter. This is normal.
- By about 2 to 4 weeks: many exclusively pumping parents build toward a daily total that meets baby’s intake, often roughly 19 to 30 oz per day (about 560 to 900 mL), with wide normal variation.
- Most babies 1 to 6 months: many stay in that same neighborhood, often around 19 to 30 oz per day (about 560 to 900 mL), but ranges are real and appetite is personal.
Connecting ounces to bottles
Every baby is different, but if your baby takes 24 oz per day and does 8 feeds, that averages about 3 oz per bottle. If they do 6 feeds, that averages about 4 oz per bottle. This is not a rule, just a planning shortcut.
If you are consistently short and baby is hungry after feeds, it is okay to use formula while you work on supply. Combo-feeding is not failure. It is a strategy.
Protecting and boosting supply
Start with the big three
- Frequency: add a session before you add minutes. An extra 10 to 15 minute pump can be more effective than extending every session.
- Effective emptying: correct flange size, good suction, and hands-on pumping (gentle breast compressions) can increase output.
- Consistency: supply responds to patterns. A few days of a solid routine often tells you more than one “bad pump.”
Use pump settings that work with your body
Higher suction is not always better. Use the highest suction that is comfortable. Pain can inhibit letdown and lead to nipple damage, which is the opposite of helpful.
Try power pumping
Power pumping mimics cluster feeding. Try it once daily for a few days if you are trying to boost supply:
- Pump 20 minutes
- Rest 10 minutes
- Pump 10 minutes
- Rest 10 minutes
- Pump 10 minutes
Do not ignore sleep, calories, and hydration
I know. Everyone says this. But it is still true: your body needs fuel and rest to make milk. You do not need a perfect diet. You do need enough overall calories, protein, and fluids so you are not running on fumes.
When to get lactation help
If you have persistent low supply despite frequent pumping, severe pain, or a baby with growth concerns, an IBCLC (lactation consultant) can help troubleshoot flange sizing, pumping technique, and medical contributors like retained placental fragments, thyroid issues, or hormonal factors.
Troubleshooting
“My output suddenly dropped”
- Check valves and membranes. These wear out and can tank suction.
- Replace tubing if it is stretched, wet, or loose.
- Reassess flange size if your nipples have changed postpartum. This happens.
- Look at timing. Dropping an overnight pump can reduce supply for some parents.
- Consider your cycle returning. Many people notice a temporary dip around ovulation or a period.
“Pumping hurts”
- Lower suction and confirm flange size.
- Use a tiny amount of pump-safe lubricant on the flange tunnel if recommended by the manufacturer.
- Treat nipple trauma like you would treat skin trauma: protect it, keep it clean, and let it heal.
Clogs and mastitis
Exclusive pumpers can be prone to clogs when milk is not draining well. Current clinical guidance treats this as an inflammation problem as much as a plumbing problem. What usually helps is calm, consistent milk removal and reducing swelling.
- Keep pumping regularly with comfortable suction. Do not try to “blast” a clog out with painful settings.
- Use ice or cold packs after pumping to reduce swelling.
- Consider an anti-inflammatory like ibuprofen if you can take it and your clinician says it is ok.
- Massage: keep it very gentle. Think light lymphatic-style sweeping strokes toward the armpit and collarbone. Avoid deep, aggressive massage or hard vibration, which can worsen inflammation and tissue damage.
Seek care urgently for fever, flu-like symptoms, rapidly worsening redness, or if you feel truly unwell. Mastitis is treatable and you do not have to push through it alone.
“I am making too much milk”
Oversupply can sound like a nice problem until you are leaking constantly and fighting recurrent clogs. Often the solution is not longer pumping. It is gradually reducing stimulation so your body gets the message. Drop minutes slowly, then consider dropping a session once you are stable. If you are prone to mastitis, taper even more slowly and consider looping your clinician in early.
Milk storage
Storage guidelines can vary slightly by organization and by your baby’s health status. If your baby is premature or medically fragile, follow your NICU or pediatric team’s instructions.
Quick safety chart (common guidance)
- Room temperature: up to 4 hours is commonly cited for freshly expressed milk
- Refrigerator (40°F / 4°C or colder): up to 4 days
- Freezer: about 6 months is ideal, up to 12 months is often considered acceptable
- Thawed in the fridge: use within 24 hours
- Warmed milk: use within 2 hours
- Label everything with date and volume.
- Use the oldest first (first in, first out).
- Mixing milk: Updated guidance supports combining freshly pumped milk with already chilled milk. If you prefer, you can still chill first, but you do not have to make it a whole extra chore.
- Freeze in smaller amounts (2 to 4 oz) to reduce waste.
- Thaw safely: thaw in the fridge or under cool-to-warm running water. Avoid microwaving due to hot spots and nutrient damage.
Soapy taste (high lipase)
If your thawed milk smells or tastes soapy and baby suddenly refuses it, it may be high lipase. It is usually still safe, just unpopular. Some families mix it with fresh milk, try different thaw methods, or talk with an IBCLC about whether scalding is appropriate for their situation.
Make it sustainable
Build a pump station you actually like
- Water bottle and snacks
- Phone charger
- Spare parts, clean burp cloth
- Hands-free pumping bra
- A small bin for dirty parts so they stop migrating across the house
Parts cleaning shortcuts
Follow your pump manufacturer’s cleaning instructions. Many parents find it helpful to have multiple sets of parts so they are not forced into middle-of-the-night sink marathons.
If you have heard about refrigerating pump parts between sessions, know that guidance differs. For healthy, full-term babies, some families use this as a convenience strategy, but it is not universally recommended. The safest approach is washing after each use. If you are considering a shortcut, ask your pediatrician, especially for preterm infants or babies with immune concerns.
Support intake cues
Use a slower flow nipple and paced feeding when possible. It can reduce choking, spit-up, and the “why is my baby suddenly demanding huge bottles?” cycle that can pressure you to pump more than needed.
Combo-feeding
Sometimes you want a little more sleep, a little more flexibility, or you are simply done fighting the math of ounces. Introducing formula can be a smart, loving choice.
To protect supply while combo-feeding:
- Keep your most productive pumps (often early morning).
- Replace missed milk removals thoughtfully. If you skip a pump regularly, your body will usually adjust downward.
- Start with one bottle per day of formula and monitor comfort. If you are prone to clogs, go slower.
If your goal is to maintain some breast milk long-term, many parents do well keeping 3 to 5 pumps per day, but your mileage may vary.
How to wean
Weaning goes best when it is gradual. Fast changes can lead to engorgement, clogs, and mastitis. Think “slow fade,” not “cold turkey.” If you have a history of oversupply or recurrent mastitis, go extra slow and consider getting medical guidance.
A simple step-down plan
- Choose one session to reduce, often the one you dread most or the one with the lowest output.
- Reduce minutes first for several days (for example, drop 2 to 5 minutes per session).
- Then drop the session once you are comfortable.
- Wait 3 to 7 days before reducing the next session.
What safe discomfort looks like
Some fullness is normal. Sharp pain, fever, chills, or a spreading red area is not. If you are getting recurrent clogs while weaning, slow down and consider talking with your clinician.
If you want to keep one pump a day
Many parents maintain a single morning or bedtime pump for a while, especially if they like providing one bottle of breast milk daily. You can taper to that rhythm, then decide when you are ready to fully stop.

When to call a clinician
- Baby has fewer wet diapers, seems lethargic, or is not gaining weight as expected
- You have fever, chills, or flu-like symptoms with breast pain
- You see pus or significant worsening redness on the breast
- Severe nipple damage or bleeding that is not improving
- Persistent low supply despite frequent pumping and good pump function
If you are in that 3 AM spiral, hear this: you do not need to solve it alone tonight. Feeding your baby is the goal, and there are many safe ways to get there.
A quick pep talk
Exclusive pumping is a lot of invisible labor. If all you did today was pump, wash parts, and keep a tiny human alive, that is not “just” anything. That is parenting at full volume.
Make the plan fit your life, not the other way around. And if you want, pick one small upgrade this week: a better flange fit, an extra set of parts, or a schedule that lets you sleep an extra hour. Tiny changes add up fast.


