Failure to Thrive in Babies and Toddlers
Sarah Mitchell
Sarah Mitchell is a Registered Pediatric Nurse and a mother of three who has spent over a decade helping families navigate the beautiful, chaotic early years of childhood. She combines evidence-based medical knowledge with real-world parenting experience to offer practical, compassionate advice. At Awesome Parent, Sarah's mission is to help exhausted parents find solutions, trust their instincts, and finally get some sleep.
If you have ever stared at a growth chart and felt your stomach drop, you are not alone. “Failure to thrive” (often shortened to FTT) is one of those phrases that sounds scarier than it needs to, especially when you are sleep-deprived and doing your absolute best.
As a pediatric nurse and a mom, I want you to know two things can be true at once: slow weight gain can be a real medical concern, and most kids who get flagged early do very well with the right plan and follow-up.

What “failure to thrive” means
FTT is not a single diagnosis. It is a clinical signal that a baby or toddler is not gaining weight as expected, or is not growing in a balanced way over time.
There is no single universal cutoff used everywhere. Different clinics and specialists use slightly different definitions, but common ways a child may be flagged include:
- Weight-for-age or weight-for-length (or BMI in older toddlers) falling very low on standardized growth charts (often below the 5th percentile)
- Crossing down two or more major percentile lines over time (more on this below)
- Poor weight gain velocity, meaning the pattern of gain is slower than expected between visits
Important: FTT is about a pattern over time, not a single off day, a single low weight, or one visit with a different scale.
One more practical note: the type of growth chart matters. In the U.S., many practices use WHO growth charts for children under 2 and CDC growth charts for ages 2 and up. Your clinic may use different standards, but your pediatrician can tell you which chart they are using and why.
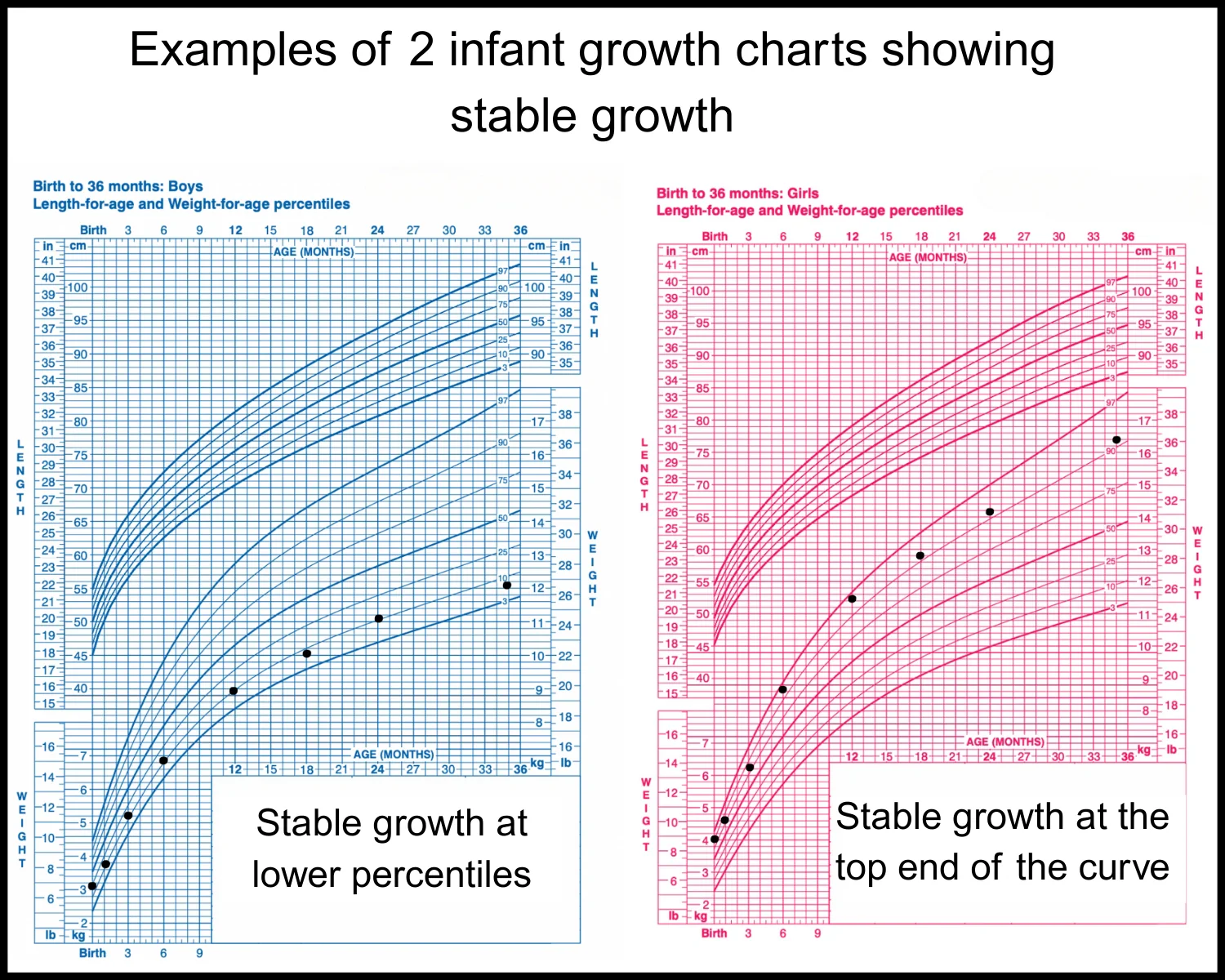
Growth charts: what matters
Growth charts can be incredibly helpful, and also incredibly confusing. Here is the simplest way to think about percentiles:
- A percentile is not a grade.
- It is a way of comparing your child’s measurements to many other children of the same age and sex.
- Healthy kids come in all sizes. A child can be perfectly healthy at the 5th percentile if they are consistently tracking there and meeting milestones.
Normal variation
These situations often end up being normal, especially if your child is otherwise thriving:
- Small, steady growth that matches family genetics (small parents often have smaller kids)
- A brief dip during an illness, followed by catch-up growth
- Measurement differences (different scale, clothing, wiggly toddler, length measured slightly differently)
- “Channeling” in early infancy, when some babies settle into a new curve in the first months of life
Crossing percentiles
Pediatricians pay closer attention when a child’s weight drops across percentile lines over multiple visits, especially if:
- Weight drops first and later length/height slows too (this is a common undernutrition pattern, but not the only one)
- There is no rebound after illness
- There are feeding struggles, vomiting, diarrhea, pain with feeding, or developmental concerns
A helpful rule of thumb: one low point does not tell the story. The trend tells the story.
If your baby was born early, ask your pediatrician if they are plotting growth by corrected age (also called adjusted age). For many preterm infants, using corrected age for a period of time gives a much more accurate picture of growth expectations.
What your pediatrician is listening for
If your child is not gaining weight well, a big part of the visit is detective work. You might feel like you are being asked a million questions. That is not judgment. That is your child’s clinician trying to pinpoint where calories may be getting lost: not taken in, not kept down, not absorbed, or burned too quickly.
Feeding questions you may hear
- Milk and formula details: Are you breastfeeding, formula feeding, or combo feeding? How often? How long? How much per feed? Are there long stretches without feeds?
- Formula mixing: What brand and type? How do you mix it? (This is a very common place where accidental under-concentration can happen.)
- Latch and transfer (breastfeeding): Pain? Clicking? Falling asleep quickly? Do you hear swallows? Any tongue-tie concerns? Have you done weighted feeds with a lactation consultant?
- Solids (older infants and toddlers): When did solids start? What does a typical day look like? Any strong preferences, gagging, or refusal?
- Mealtime structure: How many meals and snacks? How long do meals last? Are there lots of distractions? Are caregivers using pressure or “one more bite” battles?
- Liquids and grazing: How much milk, juice, sweet drinks, smoothies, or “toddler drinks” per day? Constant sipping can blunt appetite for calories from food.
- Spit-up, reflux, or vomiting: How often? Any pain, arching, feeding refusal, coughing, choking, or back-to-back respiratory infections? (Uncomplicated spit-up is very common and usually not a cause of FTT. It is reflux with poor intake, discomfort, frequent vomiting, or breathing symptoms that raises concern.)
- Stools: Frequency, consistency, greasy or very foul-smelling stools, blood, chronic diarrhea, constipation.
- Overall health and development: Recurrent illnesses (cough, wheeze, fevers, UTIs), energy level, sleep, and whether milestones are being met.
- Family and social factors: Food insecurity, caregiver stress, access to formula, complicated schedules, postpartum depression or anxiety. These questions are meant to connect you with support, not to blame. In some situations, clinicians also have to consider whether a child has enough safe access to nutrition and consistent care. When that concern comes up, the goal should still be support and protection for the child and family, not shame.
If it helps, bring a simple 3-day log of feeds and foods, plus diapers and symptoms. Not forever, just enough to give your child’s team a clear snapshot.
Common causes
Clinically, we often group contributors into a few big buckets. More than one can be true at the same time.
Also worth hearing out loud: in many babies and toddlers, the first “why” we find is something fixable, like a feeding mechanics issue, a schedule gap, or a calorie mismatch. That is exactly why the history matters so much.
1) Not enough calories going in
- Breastfeeding transfer issues (latch difficulties, low supply, inefficient feeding)
- Incorrect formula preparation or not enough total volume
- Feeding schedules that inadvertently leave long gaps
- Feeding aversion, sensory feeding issues, or significant pickiness that limits intake
- Toddler grazing on low-calorie foods and drinks
- Unintentional calorie deficits from overly restrictive or poorly planned diets (for example, unguided dairy-free diets, or vegan diets without a pediatrician or dietitian helping ensure adequate calories, protein, calcium, vitamin D, iron, and B12)
2) Calories not staying down
- Reflux with significant discomfort, feeding refusal, or frequent vomiting (again, mild spit-up alone is usually not the culprit)
- Frequent vomiting from infection or other gastrointestinal issues
- Swallowing dysfunction or aspiration concerns (coughing, choking, wet-sounding breathing during feeds)
3) Calories not being absorbed well
- Food allergies or intolerances in some children
- Celiac disease (more common after gluten has been in the diet; can show up as poor growth, diarrhea, bloating, irritability)
- Other malabsorption conditions (less common, but important when symptoms fit)
4) Calories being used up faster
- Congenital heart disease or chronic lung disease (increased work of breathing, fatigue with feeds)
- Hyperthyroidism (rare in infants and toddlers, but can cause poor weight gain with increased appetite and other signs). Thyroid concerns are evaluated based on the whole picture, and thyroid testing is typically targeted. (Hypothyroidism more often affects growth in different ways and is usually picked up through newborn screening in many settings.)
- Chronic infections or inflammatory conditions
5) Other contributors
- Prematurity or a history of being small for gestational age (some need extra time and targeted nutrition to catch up)
- Neurologic or genetic conditions affecting tone, swallowing, or coordination
- Oral-motor issues, tongue-tie, or structural differences
- Caregiving stressors, feeding dynamics, or access to adequate nutrition

What evaluation looks like
Most pediatricians start with the least invasive, most practical steps first: confirm measurements, assess feeding, and schedule close follow-up.
Step 1: confirm growth data
- Weight measured on the same type of scale when possible
- Baby undressed to a dry diaper for consistency
- Length measured carefully (it is surprisingly easy to under-measure length, which can distort weight-for-length)
Step 2: exam and targeted questions
Your clinician will look for clues like dehydration, oral thrush, heart murmurs, respiratory effort, muscle tone, skin changes, abdominal findings, and signs of nutritional deficiencies.
Step 3: a plan and short follow-up
Follow-up is often sooner than parents expect, sometimes in 1 to 2 weeks for infants. This is not because anyone is panicking. It is because short intervals help us see whether the plan is working.
What “adequate” weight gain looks like depends on age, feeding method, and the child’s medical history, so your pediatrician may not give one single number that fits every situation. Instead, they will watch your child’s trend and whether your child is meeting the goals you set together.
Depending on age and feeding method, a plan might include:
- Increasing feeding frequency or offering an extra feed
- Supporting breastfeeding (lactation consult, pumping plan, weighted feeds)
- Adjusting formula concentration only under medical guidance
- For older babies and toddlers: adding calorie-dense foods (avocado, oils, full-fat yogurt, cheese, eggs, nut butters when safe) and creating predictable meal and snack times
- Limiting appetite-killing liquids (like too much milk or juice) when appropriate
Quick safety notes for calorie boosters:
- Honey is not safe under 12 months.
- Whole nuts are a choking hazard for young children. Nut butters should be offered in age-appropriate forms (thinly spread, mixed into yogurt or oatmeal, or thinned) based on your pediatrician’s guidance.
- Follow your pediatrician’s advice on allergy introduction, especially if your child has eczema or known food allergies.
Step 4: tests when indicated
Not every child needs bloodwork. When symptoms or exam findings point to a medical cause, the pediatrician may order targeted tests. Examples can include:
- Blood tests to check for anemia, inflammation, or metabolic concerns
- Urine testing if urinary tract infection is suspected
- Stool testing if malabsorption is a concern
- Condition-specific tests, such as screening for celiac disease in the right age and symptom context
The key word is targeted. A “kitchen sink” approach is rarely the first move.
Referrals and early support
When a child needs extra support, referrals are not a failure. They are a shortcut to the right tools.
Common referrals
- Registered dietitian (pediatric): helps calculate needs and build a realistic plan for your child’s schedule, preferences, and budget
- Lactation consultant: evaluates latch, milk transfer, supply support, and pumping strategy
- Feeding therapy (speech-language pathologist or occupational therapist): helpful for oral-motor delays, swallowing concerns, sensory feeding issues, and feeding aversion
- Pediatric gastroenterology: for persistent vomiting, diarrhea, blood in stool, suspected malabsorption, or unclear cases
- Pediatric cardiology or pulmonology: if there are signs of increased work of breathing, fatigue with feeds, or concerning exam findings
- Early intervention services: for children under 3 with developmental delays, low tone, or feeding skills concerns (often available through community programs)
What early intervention can involve
- Coaching on positioning and pacing during feeds
- Building tolerance for textures and reducing gagging
- Creating a low-pressure mealtime routine
- Supporting motor skills that affect feeding (sitting stability, hand-to-mouth coordination)
These supports are practical, skill-based, and very parent-friendly when done well.
When to call urgently
Please seek urgent medical care if your baby or toddler has poor weight gain plus any of the following:
- Signs of dehydration (very few wet diapers, dry mouth, no tears, sunken soft spot in a young infant, unusual sleepiness)
- Difficulty breathing, fast breathing, or working hard to breathe
- Repeated vomiting, green vomit, or vomiting with a swollen belly
- Blood in stool or black, tarry stools (jet-black, sticky, and foul-smelling can signal bleeding). Note: iron supplements can darken stools too, but if you are not sure, it is worth a call.
- Lethargy, limpness, or a baby who is hard to wake
- Fever in a young infant: a rectal temperature of 100.4°F (38°C) or higher in babies under 3 months needs urgent medical evaluation. If your baby is older, follow your pediatrician’s age-specific guidance.
If you are unsure, call your pediatrician’s after-hours line. That is exactly what it is there for.
What you can do now
If you are worried about your child’s growth, these steps are both safe and useful:
- Schedule a weight check rather than relying on a home scale. Clinic measurements are more consistent.
- Bring a simple feeding log for 3 days (times, amounts, foods, vomiting, stools).
- Write down your top 5 concerns before the visit. Sleep deprivation steals our ability to remember details.
- Ask for the plan in writing: what changes to try, what goal they are watching, and when you will recheck.
And from one parent to another: if you have been coaxing, bargaining, and googling at 3 AM, you are not doing anything wrong. You are responding to a real stressor. With a clear plan and close follow-up, most families start to feel grounded again quickly.
If your gut says something is off, you deserve a thorough, calm evaluation. No shame, no drama, just good medicine and practical support.
Quick FAQ
Can a baby be healthy at a low percentile?
Yes. Many healthy babies track consistently at a lower percentile. What raises concern is dropping percentiles over time or signs that a child is not getting enough nutrition or has an underlying condition.
Will my child catch up?
Often, yes, especially when the cause is feeding mechanics, intake, or a temporary medical issue. Catch-up growth is something your pediatrician monitors carefully to ensure it is steady and safe.
Should I switch formulas or start supplements on my own?
Talk with your pediatrician first. Some changes help, others can backfire or mask the real issue. The safest approach is a guided plan with close follow-up.