Lip Tie in Babies
Sarah Mitchell
Sarah Mitchell is a Registered Pediatric Nurse and a mother of three who has spent over a decade helping families navigate the beautiful, chaotic early years of childhood. She combines evidence-based medical knowledge with real-world parenting experience to offer practical, compassionate advice. At Awesome Parent, Sarah's mission is to help exhausted parents find solutions, trust their instincts, and finally get some sleep.
If you are staring at your baby’s upper lip at 2 AM wondering, “Is that little piece of tissue the reason feeding is such a struggle?”, you are not alone. I met countless families in clinic who were exhausted, worried, and getting wildly conflicting advice online. Let’s slow it down and talk about what a lip tie is, what it can (and cannot) explain, and what treatment options actually look like.
Quick note: This article is for education and support, not medical advice. If your baby is not feeding well or not gaining weight, loop in your pediatrician promptly.

What is a lip tie?
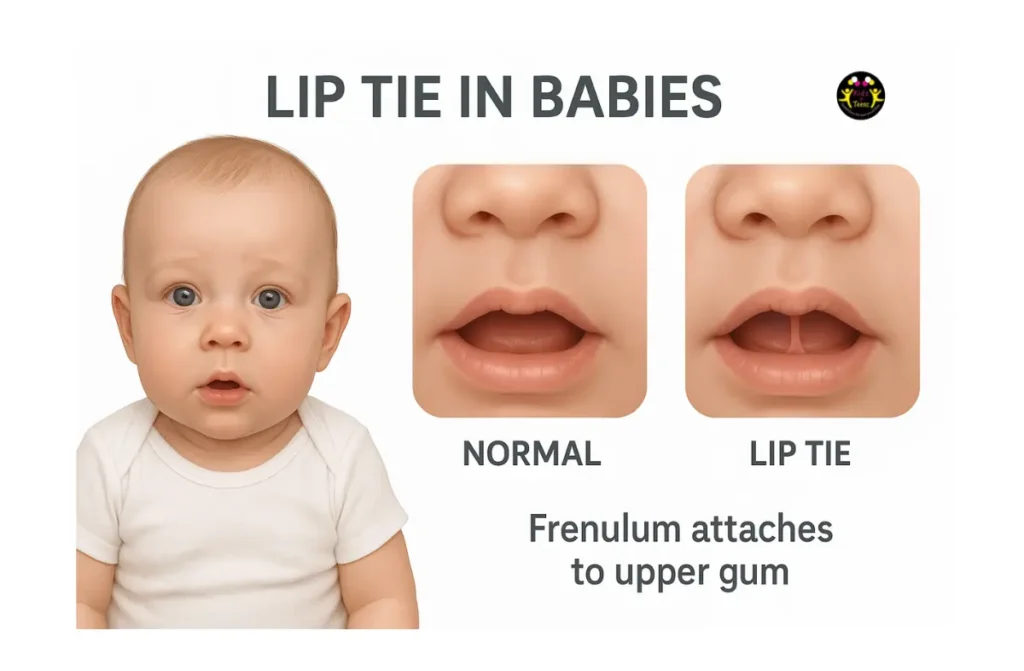
A lip tie usually refers to a tight or restrictive upper labial frenulum, which is the thin band of tissue connecting the inside of the upper lip to the gum above the top front teeth.
Almost all babies have a visible frenulum. That is normal anatomy. A lip tie becomes a concern when the tissue is positioned or tight enough that it seems to limit the upper lip’s ability to flange outward (think “fish lips”) during feeding, or it contributes to ongoing feeding problems despite good positioning and support.
Signs parents notice
Lip tie is often discussed in the context of breastfeeding, but it can show up with bottle feeding too. The tricky part is that many of these signs can also come from latch technique, oversupply, reflux, bottle flow issues, suck swallow breathe coordination, oral motor immaturity, tongue tie, or simply a baby who is still learning.
Possible signs
- Upper lip tucks inward during feeds and is hard to gently flip outward
- Shallow latch that keeps popping on and off the breast or bottle nipple
- Clicking sounds while feeding (loss of seal)
- Milk leaking from the corners of the mouth
- Prolonged feeds, frequent relatching, or baby seeming frustrated at the breast or bottle
- Gassiness and increased air swallowing due to a poor seal
- Nipple pain or damage for the breastfeeding parent, especially if other latch adjustments have not helped
What you might see if you gently lift the lip
- A frenulum that appears thick, tight, or short
- The upper lip may look like it is pulled down toward the gum when lifted
- In some babies, the frenulum attaches low and extends close to where teeth will later emerge
Important: Seeing a prominent frenulum does not automatically mean feeding problems are being caused by a lip tie. A photo can be misleading. A functional feeding assessment tells you far more than appearance alone.
Lip tie vs tongue tie
Lip tie involves the upper lip’s attachment to the gum. Tongue tie involves the tissue under the tongue (lingual frenulum) restricting tongue movement.
- Tongue tie can be more directly linked to ineffective milk transfer because the tongue has to elevate, extend, and cup to feed well. Evidence and diagnostic criteria vary, so assessment matters.
- Lip tie is more controversial because many babies feed well with a visible or low attaching upper frenulum, and the research on lip tie as a stand alone cause of feeding problems is less clear.
In real life, some babies have both. When feeding is difficult, a qualified clinician should assess structure and function of the tongue, lips, jaw, palate, and overall latch.
Lip tie grades
You may hear about “grade 1, 2, 3, 4” lip ties. Several grading systems exist (the Kotlow scale is commonly referenced online), and they typically describe where the frenulum attaches on the gum.
Here is the part I want you to remember: appearance based grades have limited correlation with feeding function, can vary between examiners, and are not validated predictors of feeding outcomes on their own.
That said, here is a parent friendly way to understand what people usually mean by the grades:
Grade 1
The frenulum attaches higher on the gum. Many babies with this appearance lift the lip easily and feed well.
Grade 2
The frenulum attaches a bit lower on the gum. Some babies still flange well and feed perfectly. Others may struggle, especially if there are additional factors like a high palate, tension, or tongue restriction.

Grade 3
The frenulum attaches close to where the front teeth will erupt. The upper lip may look tethered on exam, but function can still vary widely from baby to baby.

Grade 4
The frenulum appears to extend to the very front of the gum and can look quite tight. Even with this look, the key question is still: is it affecting function?

My nurse take: Grades can help clinicians describe anatomy, but they do not diagnose a feeding problem. If someone is diagnosing from a single photo, you deserve a better evaluation.
What the evidence says
Parents deserve honesty here. Research on isolated upper lip tie and whether releasing it reliably improves feeding is limited and mixed. Many experts emphasize that feeding outcomes depend on the whole picture: latch, milk flow, tongue function, palate shape, oral motor skills, and support.
This is also why you may see big differences in who gets diagnosed and who gets offered a procedure. If you feel pressured, confused, or unsure, it is reasonable to ask for a second opinion from a clinician who watches a full feed and assesses function.
Breastfeeding and lip tie
During breastfeeding, the upper lip helps form a comfortable seal on the breast while the tongue and jaw do most of the work. If the upper lip cannot flange outward, some babies compensate with a shallower latch.
Possible breastfeeding issues
- Painful latch that does not improve with positioning help
- Blanched, creased, or “lipstick-shaped” nipple after feeds
- Frequent unlatching and fussing at the breast
- Slow weight gain or falling off growth curve when milk transfer is poor
- Oversupply symptoms can mimic tie issues too, so it is worth sorting out
If your baby is gaining weight well and feeds are comfortable, a visible upper frenulum is usually just normal anatomy.
Bottle feeding and lip tie
Bottle feeding can also be affected by seal and oral motor coordination. Some clinicians and parents report that a very restrictive upper lip may make it harder for a baby to maintain suction, but evidence linking an isolated upper lip tie to bottle feeding problems is limited.
Possible clues
- Clicking and losing the latch on the bottle nipple
- Milk dribbling from the corners of the mouth
- Very gassy after feeds or frequent burping needs
- Taking a long time to finish a bottle, or acting tired partway through
Before blaming the frenulum, check the basics: nipple flow rate, bottle shape, paced feeding, upright positioning, and whether baby is clamping due to stress or fast flow.
When to get checked
If feeding is painful, stressful, or your baby is not gaining weight as expected, it is worth getting a careful assessment. The best evaluations look at function and not just anatomy.
Who can help
- Pediatrician to evaluate growth, hydration, reflux, and rule out other issues
- IBCLC lactation consultant for latch, positioning, milk transfer, and a full feeding assessment
- Pediatric ENT, pediatric dentist, or oral surgeon for tie assessment and discussing revision if appropriate
- Speech-language pathologist or feeding therapist (infant feeding specialty) when oral motor issues are suspected
Bring this to your appointment
- Baby’s feeding pattern (how often, how long, how many ounces if bottle feeding)
- Diaper counts and any weight checks you have
- What you have tried (positions, nipple shields, bottle nipples, paced feeds)
- Photos or short videos of a typical feed if your clinician allows it
Do all lip ties need revision?
No. In many babies, an upper lip frenulum that looks dramatic is still flexible enough that feeding is fine. And for babies with feeding issues, lip tie may be one piece of a bigger puzzle.
Revision is usually considered when
- There are significant feeding symptoms (pain, poor milk transfer, poor weight gain) and
- Skilled lactation support and feeding adjustments have not resolved the issue and
- A clinician finds a functionally restrictive frenulum on exam during a full feeding assessment
You may also hear about lip ties in relation to future tooth spacing or a gap between the front teeth. For most children, that gap often changes naturally as teeth erupt. Decisions about revising a lip frenulum for dental reasons are typically made later and with a pediatric dentist or orthodontic input, not in the newborn stage unless feeding is affected.
Frenotomy vs frenectomy
A procedure to release the frenulum may be called a frenotomy or frenectomy. People often use these words interchangeably, but technically:
- Frenotomy is a cut or release
- Frenectomy is removal of tissue (or a more extensive release)
In everyday conversation you may also hear “lip tie revision.” There is not one universal standard for how this is done, so it is fair to ask exactly what your provider means.
Common approaches
- Scissors release in the office
- Laser release (often in a dental setting)
In young infants, it is often a quick procedure. Pain control and protocols vary widely by clinician, age, and setting. Options may include topical anesthetic, local anesthetic, and comfort strategies like swaddling and sucrose. Some providers avoid certain anesthetics in young infants. Ask what your provider uses, what they recommend for your baby’s age, and what you should expect that day.
What parents typically see afterward
- A small wound area inside the upper lip
- Some fussiness for a short period
- A small amount of bleeding is possible right after the release
- Feeding may improve quickly, or it may take days to weeks as baby relearns latch patterns
Risks to discuss
- Bleeding, infection (rare), pain
- Reattachment or scarring
- No improvement if the frenulum was not the primary cause
If someone is promising instant, guaranteed results, take a breath and ask more questions. Bodies are not vending machines.
Aftercare and support
After a release, some providers recommend specific stretching or massage exercises, while others emphasize feeding therapy and optimizing latch without aggressive stretching. Recommendations vary, and evidence is still evolving. The most important thing is that you have a clear plan and follow up.
Helpful supports
- Follow up with an IBCLC within a few days to rebuild a deeper latch
- Paced bottle feeding if bottle feeding, to reduce gulping and air intake
- Short, calm practice sessions when baby is not overly hungry
- Ask your clinician when to seek help for bleeding, fever, poor feeding, or dehydration
Call the doctor now
Feeding struggles can turn into dehydration faster than most parents expect, especially in young infants. Call your pediatrician urgently or seek urgent care if you notice:
- Fewer wet diapers than expected for age, very dark urine, or a dry mouth
- Sleepiness that makes it hard to wake baby for feeds
- Fast breathing, persistent vomiting, or signs of respiratory distress
- Weight loss beyond what your pediatrician considers normal, or no weight gain
- After a procedure: bleeding that does not stop with gentle pressure and feeding, or any concern your baby is not acting right
Quick diaper guide
- Day 1: at least 1 wet diaper
- Day 2: at least 2 wet diapers
- Day 3: at least 3 wet diapers
- Day 4: at least 4 wet diapers
- Day 5 and onward: typically 6 or more wet diapers per day
These are general benchmarks. Always follow your pediatrician’s guidance, especially for preterm infants or babies with medical conditions.
Quick checklist
- Start with a feeding assessment (IBCLC for breastfeeding, feeding therapist if bottle feeding difficulties persist).
- Check the basics: positioning, paced feeds, bottle nipple flow, and burping strategies.
- Track output and weight: diapers and a weight check tell the truth when feeds feel confusing.
- Ask about tongue function: lip tie and tongue tie can coexist, and tongue restriction is often more impactful.
- Consider revision only if restriction is clearly affecting function and symptoms persist despite support.
If you are in the thick of this right now, I want you to hear this clearly: you are not failing. Feeding is a skill for both of you, and getting the right help is a strong, loving move.
FAQ
Can a lip tie cause reflux?
A restrictive latch can lead to air swallowing, which can increase spit ups and discomfort. Symptoms like fussiness, back arching, and frequent spit up are nonspecific and can have many causes, including normal newborn behavior. If symptoms are severe, painful, or weight gain is affected, check in with your pediatrician.
Will a lip tie stretch on its own?
Many frenula change in appearance as babies grow. What matters most is how your baby feeds and grows over time, not whether it “looks tight” in a photo.
Is a release always painful?
Babies may cry during and after for a short time, and discomfort varies. Pain control protocols differ by setting. Ask your provider what they use for comfort and what to expect in the first 24 hours.
Is it better to revise early?
If a release is truly needed for feeding, earlier intervention can sometimes help families protect milk supply and improve feeding efficiency. But early is not automatically better if the diagnosis is uncertain. Start with a solid functional assessment and do not be afraid to seek a second opinion if you feel unsure.