MRSA Skin Infections in Kids: What They Look Like
Sarah Mitchell
Sarah Mitchell is a Registered Pediatric Nurse and a mother of three who has spent over a decade helping families navigate the beautiful, chaotic early years of childhood. She combines evidence-based medical knowledge with real-world parenting experience to offer practical, compassionate advice. At Awesome Parent, Sarah's mission is to help exhausted parents find solutions, trust their instincts, and finally get some sleep.
If you are staring at your child’s “pimple” at 11 pm wondering why it keeps getting bigger, you are not alone. In pediatric triage, skin bumps are a very common reason parents call, mostly because they can look deceptively similar at first.
Here is the calm, practical truth: many bumps are minor and treatable at home. But some skin infections, including MRSA, can worsen quickly and need medical care. This guide will help you compare what you are seeing, know what is safe to do tonight, and recognize the red flags that mean “do not wait.”

First, what is MRSA?
MRSA stands for methicillin-resistant Staphylococcus aureus. Staph bacteria commonly live on skin and in noses without causing problems. When staph gets into a tiny break in the skin, it can cause an infection. MRSA is a type of staph that is resistant to some common antibiotics, so it may require a different antibiotic if medicine is needed.
In kids, community-acquired MRSA most commonly shows up as a skin abscess (a boil) or can contribute to cellulitis (a spreading skin infection).
Important nuance: drainage is about how abscesses work, not just about MRSA. Any abscess can be hard for antibiotics to penetrate because pus is “walled off.” Small boils sometimes improve with warm compresses and may drain on their own, but many still need a clinician to drain them.
MRSA vs pimple vs impetigo
Skin infections do not read textbooks, so there is overlap. But these patterns are helpful.
1) A routine pimple or irritated hair follicle
- Size: usually small, often under the size of a pea
- Look: a tiny whitehead or red bump around a pore or hair
- Feel: mildly tender, not usually intensely painful
- Speed: tends to peak and improve over a few days
- Child seems well: no fever, normal energy
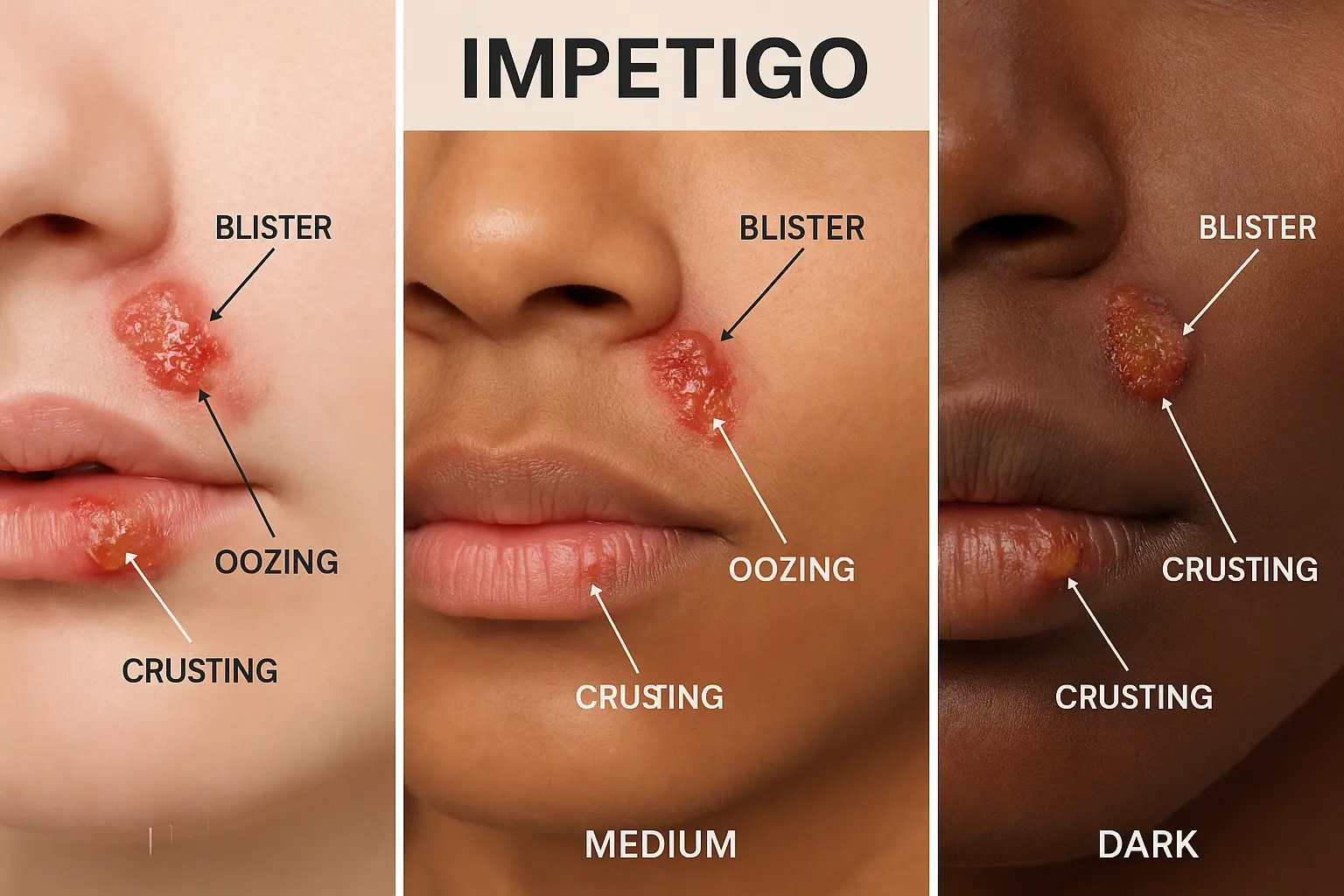
2) Impetigo (often after a cold or a scratch)
- Look: superficial sores or blisters that break open and form honey-colored crusts
- Location: common around the nose and mouth, also on arms or legs
- Itch more than pain: can be itchy and bothersome
- Spreads easily: to siblings or across the child’s skin via scratching
Note: Impetigo can be caused by staph or strep. Some cases involve MRSA, but classic impetigo is usually more “crusty and superficial” than “deep, swollen, and walled off.”
3) MRSA abscess (boil): the “spider bite” look-alike
- Look: a red, swollen, warm bump that often becomes a pus-filled pocket
- Feel: more painful than you would expect for the size
- Center: may develop a white or yellow head or a darker “plug”
- Firm then squishy: can start hard, then become fluctuant (like there is fluid under the skin)
- Grows fast: may enlarge noticeably over 24 to 48 hours
4) Cellulitis: the spreading redness that matters
Cellulitis is an infection of the deeper skin layers. It may happen with or without a clear abscess.
- Look: a spreading area of redness, warmth, and swelling
- Edges: often less defined, “moving outward”
- Pain: tender and sore to touch, sometimes throbbing
- Fever or feeling ill: more common than with a simple pimple
Is it contagious?
Yes, impetigo is contagious. MRSA can also spread through skin-to-skin contact and through shared items like towels, razors, uniforms, or bedding.
That said, you do not need to panic-clean your house top to bottom at 2 am. Focus on the high-impact steps:
- Keep the area covered with a clean, dry bandage.
- Handwashing for everyone, especially after bandage changes.
- Do not share towels, washcloths, clothing, sports gear, or bedding until improving.
- Launder clothing and linens normally. If you want an extra margin, use the warmest appropriate water setting for the fabric and dry thoroughly.
- Trim nails and discourage picking or squeezing.
Safe home care tonight
If your child is otherwise well and the spot is small, these steps are generally safe:
Warm compresses
Apply a warm, damp compress for 10 to 15 minutes, 3 to 4 times per day. Warmth can improve blood flow and sometimes helps a small boil come to a head and drain on its own.
Clean gently
- Wash with mild soap and water.
- Pat dry, then cover.
- Avoid harsh scrubbing. Also avoid repeated use of hydrogen peroxide or alcohol on open skin, since these can irritate tissue and slow healing.
Do not pop it
I know it is tempting, especially if it looks like a large pimple. But squeezing can push bacteria deeper, worsen cellulitis, and increase scarring. It also spreads germs onto hands and surfaces.
Pain and fever support
If your child is uncomfortable, you can use age-appropriate fever and pain medicine (acetaminophen or ibuprofen, if they can take it). Follow label dosing or your pediatrician’s guidance.
Track changes
- Mark the edge: If there is a red patch around the bump, lightly mark the outer edge with a pen. If the redness grows past the line over a few hours, that is useful information for urgent care.
- Take a quick photo: A clear photo in good light can help if you use telehealth or need to compare size in the morning.
- Check temperature: If your child feels warm or seems unwell, take an actual temperature and write it down.
One more practical note: topical ointment alone will not treat a deep abscess. If this looks like a boil with a pus pocket, warm compresses and medical evaluation are more useful than trying to “cream it away.”
What care may involve
Many abscesses improve only after the pus pocket is drained. Antibiotics alone sometimes cannot penetrate a walled-off pus pocket well.
Incision and drainage (I&D)
Parents often picture something dramatic. Most pediatric I&Ds are quick and routine.
- Numbing: the clinician typically uses a numbing medicine. For younger kids or very anxious kids, some clinics use additional comfort measures.
- Opening the abscess: a small opening lets pus drain out.
- Culture: they may swab the drainage to see what bacteria grows and which antibiotics work best.
- Packing: sometimes a small strip of gauze is placed to keep it draining, but not always.
- Aftercare: you will get instructions for warm compresses, dressing changes, and follow-up.
It is normal for the area to look a bit more inflamed right after drainage. Most kids feel noticeably better within 24 to 48 hours once pressure is relieved.
When are antibiotics added? Your clinician decides based on the full picture. Antibiotics are more likely if there is fever, spreading cellulitis, multiple lesions, very young infants, immune suppression, or certain high-risk locations. Sometimes I&D alone is enough for a small, uncomplicated abscess.

Call today vs urgent care
If you are on the fence, these are good “get medical advice today” situations:
- The bump is getting bigger over 24 to 48 hours.
- It is very painful, firm, or hot.
- There is a visible pus pocket or it looks like a boil.
- Redness is spreading beyond a small rim around the bump.
- Your child has eczema, diabetes, immune suppression, or a history of MRSA.
- The infection is on the face, near the eye, on the hand, genitals, or over a joint.
- Your child is a wrestler, plays close-contact sports, or shares equipment, and you suspect a contagious skin infection.
What to do: Call your pediatrician today if possible. If you cannot be seen promptly or it is after hours, urgent care is a reasonable next step.
Even if you end up not needing drainage, it is worth having eyes on it. Skin infections are one of those issues where earlier treatment can prevent a bigger problem.
Go to the ER now
Please seek emergency care if you notice any of the following:
- Fever with a rapidly spreading red area
- Red streaks traveling away from the spot
- Severe pain out of proportion to how it looks
- Fast worsening over hours, not days
- Significant swelling of an arm, leg, hand, foot, or around the eye
- Face or eye involvement, especially swelling of the eyelid or pain with eye movement
- Lethargy, confusion, trouble breathing, or your child “just looks really sick”
- Signs of dehydration (very dry mouth, no tears, peeing much less)
- An infant under 3 months with fever, or a young baby with a concerning skin infection
Trust your instincts here. Parents are often right when they say, “This is not my kid.”
Antibiotics
Not all skin infections need antibiotics, and not all antibiotics work for MRSA. If your child’s clinician suspects MRSA, they may choose an antibiotic that covers it, based on local resistance patterns and your child’s age and allergies.
Two important reminders:
- Do not use leftover antibiotics from another illness.
- If antibiotics are prescribed, take them exactly as directed, and return if symptoms are not improving within the timeframe you were given.
Prevent spread at home
Once you are dealing with a boil or impetigo, your goals are: contain drainage, keep hands clean, and reduce skin irritation.
- Cover draining areas with gauze and tape or a well-fitting bandage.
- Put used bandages in a small bag before tossing.
- Clean high-touch bathroom surfaces regularly.
- Have your child use their own towel and washcloth.
- For athletes: shower after practice, wash uniforms after each use, and do not share protective gear.
Back to school or daycare?
Policies vary, but many schools allow return when the lesion can be fully covered and the child can keep hands off it. For impetigo, many clinicians recommend staying home until 24 hours after starting antibiotics or until lesions are crusted and covered. If you are unsure, call the school nurse and your pediatrician.
FAQ
Can MRSA look like a bug bite?
Yes. Parents often describe it as a “spider bite” because it starts as a red, swollen bump. What raises suspicion is rapid growth, significant pain, warmth, and pus.
If it drains on its own, do we still need to be seen?
Often, yes, especially if there is spreading redness, fever, or significant pain. A clinician may want to culture it, ensure it is draining adequately, and decide if antibiotics are needed.
Will my whole family get MRSA now?
Not necessarily. With good hand hygiene, covering the area, and not sharing personal items, many families avoid spread. If multiple family members keep getting boils, ask your pediatrician about a decolonization plan and whether cultures are appropriate.
Bottom line
If you are deciding between “this is just a pimple” and “this is something bigger,” focus on pain, rapid growth, pus, spreading redness, and fever. Those are the clues that point toward an abscess or cellulitis and a need for prompt medical care.
And if you needed someone to say it plainly: you are not overreacting by getting a worsening boil checked. Skin infections are easier to treat when we catch them early, and you deserve to sleep without watching the redness creep outward.