A parent-friendly guide to Sever’s disease: why heel pain flares with sports, how it differs from growing pains, what helps at home, shoe and insert tips, ...
Osgood-Schlatter Disease in Kids: Knee Pain in Active Children
Sarah Mitchell
Sarah Mitchell is a Registered Pediatric Nurse and a mother of three who has spent over a decade helping families navigate the beautiful, chaotic early years of childhood. She combines evidence-based medical knowledge with real-world parenting experience to offer practical, compassionate advice. At Awesome Parent, Sarah's mission is to help exhausted parents find solutions, trust their instincts, and finally get some sleep.
If your child is suddenly grabbing the front of their knee after soccer practice or wincing on the stairs, you are not alone. Osgood-Schlatter disease is a common cause of front-of-knee pain in active kids and teens. The pattern is usually straightforward: a growing body, a busy sports schedule, and a spot just below the kneecap that gets irritated from repeated pulling.
As a pediatric nurse and a mom who has iced more knees than I can count, I will tell you the good news first. Osgood-Schlatter is usually manageable at home, it is not contagious, and most kids improve as they finish growing (though the bump can stick around, and a small number have symptoms that linger longer).
Quick note: This is general education, not a diagnosis. If you are unsure what is causing your child’s pain, or you see any red flags, get them checked.
What it is
Osgood-Schlatter disease is an overuse injury at a growth plate. Specifically, it affects the bony bump at the top of the shinbone (tibia) where the patellar tendon attaches, called the tibial tubercle.
Here is the simple version of what is going on:
- Kids have growth plates, which are areas of developing bone that are softer and more vulnerable than adult bone.
- The quadriceps muscle on the front of the thigh connects to the kneecap (patella) and then to the shinbone via the patellar tendon.
- When your child runs, jumps, kicks, squats, or climbs, that tendon repeatedly pulls on the growth plate.
- During a growth spurt, the bones lengthen quickly and the muscles and tendons can feel tight. That extra tightness increases the tugging and irritation.
Over time, the body may respond by building extra bone at the attachment point, which is why some kids develop a noticeable bump below the kneecap.
Who gets it most
- Most common in active kids during rapid growth, often around ages 9 to 14 (often earlier in girls than boys).
- It can affect one knee or both.
Common triggers
Anything with lots of jumping, sprinting, cutting, and kicking can set it off, especially when practices ramp up quickly or your child is doing the same motion year-round.
Sports that often flare it
- Soccer
- Basketball
- Volleyball
- Gymnastics and dance
- Track and field (sprinting, hurdles)
- Football
- Baseball and softball (especially catchers who squat a lot)
- Martial arts
- Skateboarding and activities with repeated jumping
It can also flare with everyday stuff like stairs, running around at recess, or a sudden return to activity after a break.
Training load and gear
- Avoid sudden jumps in training (extra tournaments, new private training, doubling practices).
- Supportive shoes and rotating out worn footwear can help reduce overall stress through the legs, especially on hard surfaces.
- If possible, mix in lower-impact days between high-impact sessions.

Symptoms
Osgood-Schlatter has a pretty classic symptom picture. Parents often tell me, “They can still walk, but they complain after practice,” or “It is worse when they kneel.” That is the pattern.
Most common symptoms
- Pain and tenderness at the bony bump just below the kneecap
- Swelling or puffiness in that same spot
- Pain that worsens with activity and improves with rest
- Pain with kneeling, squatting, jumping, sprinting, or climbing stairs
- A hard bump that can become more noticeable over time
- Tight quads or hamstrings
Not sure if it is Osgood-Schlatter?
Because “knee pain” is a big umbrella, here are a few clues that can help you decide what to do next. This is not a diagnosis tool.
- Patellar tendinitis (jumper’s knee): pain is usually more directly below the kneecap along the tendon, not as focused on the bony bump of the shinbone. It is more common in older teens and adults, but kids can get it too.
- Patellofemoral pain: discomfort often feels behind or around the kneecap and can worsen with stairs or sitting with knees bent for a long time. Tenderness is not as pinpointed on the tibial bump.
- Sever’s disease: another growth-plate overuse injury, but it is in the heel, not the knee.
- Meniscus injury: more likely after a twist, with swelling in the knee joint, locking, catching, or difficulty fully straightening the knee.
- ACL or ligament injury: usually a clear injury event with a pop, immediate swelling, instability, or inability to continue playing.
- Infection: fever, redness, warmth, severe pain, and a child who looks unwell is a very different picture and needs urgent evaluation.
If your child has a major limp, cannot bear weight, has fever, or the knee is rapidly swelling, skip the home-care phase and get same-day care.
Home care
The goal is to calm down the irritated attachment point while keeping your child safely active. Total couch rest is rarely necessary, but trying to push through every practice usually backfires.
1) Adjust activity
- Cut back on pain-triggering moves for a few weeks: repetitive jumping, sprint intervals, deep squats, and lots of kicking.
- Use pain as a guide: mild discomfort during activity can be okay, but pain that causes limping, changes mechanics, or lingers strongly into the next day means the load is too high.
- Try a simple rule: aim to keep pain at 3 out of 10 or less during activity, and ideally back close to baseline by the next morning.
- Swap in lower-impact conditioning if available: swimming, cycling with low resistance, or upper-body and core work.
- Avoid kneeling directly on the bump. If your child must kneel, use a cushion or knee pad.
2) Ice after activity
Ice can reduce pain and swelling.
- Apply a cold pack to the painful area for 10 to 20 minutes after sports or during flares.
- Use a thin cloth barrier to protect the skin.
- Check the skin every few minutes and stop if there is burning, numbness, or unusual discoloration.
3) Pain relief, when appropriate
For some kids, short-term pain relief helps them move more comfortably and sleep better.
- Ibuprofen or naproxen can help with pain and soreness if your child can take NSAIDs safely.
- Acetaminophen can help with pain if NSAIDs are not a good fit.
Always follow the dosing on the label for your child’s age and weight, and check with your clinician if your child has kidney disease, bleeding disorders, stomach ulcers, is on blood thinners, or has other medical complexities.
4) Stretching and strengthening
Tight quads and hamstrings increase the tug on the growth plate. A consistent, gentle routine is often the difference between recurring flares and a calmer season.
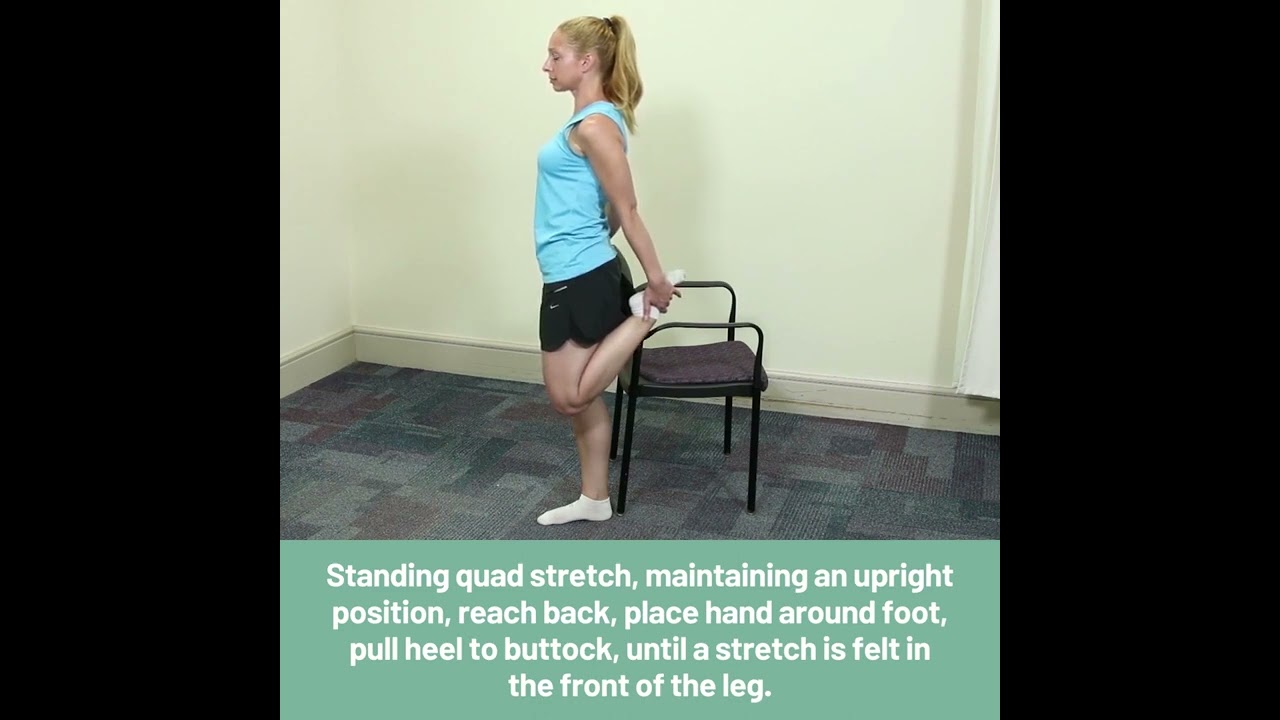
Stretching
- Gentle quad stretches daily, especially after warm muscles (after a warm shower or after practice).
- Hamstring and calf stretches to improve overall leg flexibility.
Strengthening (common PT picks)
- Straight-leg raises (quad strength without deep knee bending)
- Side-lying leg lifts or banded lateral walks (glute med and hip stability)
- Step-ups to a low step (controlled quad and hip work)
- Wall sits only if they are tolerated without bump pain
If stretching or strengthening causes sharp pain at the bump, back off and ask a physical therapist for a customized plan.

Straps and sleeves
Supportive gear does not cure Osgood-Schlatter, but it can reduce symptoms by decreasing the pull on the tendon during activity. It helps some kids more than others.
What may help
- Patellar tendon strap (often called an infrapatellar strap): worn just below the kneecap during sports. Many kids find it takes the edge off.
- Knee sleeve: can provide warmth and a sense of stability. Helpful for some kids.
- Padding for kneeling: volleyball knee pads or simple cushioning can prevent direct pressure on the tender bump.
Fit tips
- A strap should feel snug but should not cause numbness, tingling, color change, or increased pain.
- If your child’s pain is worse while wearing it, stop and reassess the fit or try a different option.
When to see a clinician
Even when the pattern sounds like Osgood-Schlatter, it is worth checking in if pain is limiting your child’s life, lasting longer than expected, or you are not sure what you are dealing with.
Make an appointment if:
- Pain persists for more than 2 to 4 weeks despite reduced activity and home care
- Your child is limping or avoiding weight-bearing
- The knee pain is affecting sleep or normal daily activity
- The diagnosis is uncertain, symptoms are on both sides and worsening, or you are worried
- Your child needs a plan to stay in sports safely (physical therapy can be a big help)
Clinicians often diagnose Osgood-Schlatter based on history and exam. X-rays are not always needed but may be used if the story is atypical, severe, or there is concern for another issue.
Red flags
Most Osgood-Schlatter cases are not emergencies. That said, knee pain in kids should be taken seriously when it looks like an injury, infection, or a joint problem.
Seek urgent care or same-day evaluation if your child has:
- Severe pain after an injury, especially if they cannot bear weight
- Significant swelling of the whole knee (not just the bump below it), especially if it comes on quickly
- Obvious deformity, knee that looks out of place, or a suspected fracture
- Fever, or the area is red, hot, and very tender
- Warmth and swelling with a child who looks ill or is unusually fatigued
- Numbness, tingling, or a foot that looks pale or cold
- Locking (cannot fully straighten or bend), repeated giving way, or instability
If you are on the fence, trust that parent gut feeling and get it checked.
How long it lasts
Osgood-Schlatter often comes and goes. Many kids have flare-ups for months, especially during growth spurts or intense seasons, and then it gradually settles as the growth plate closes.
- Short term: symptoms may improve in weeks with reduced load, ice, and stretching.
- Long term: it can take months to fully calm down, with occasional flares.
- That bump may remain: the tibial tubercle can stay prominent even after pain resolves. It is usually just a cosmetic change, but a small number of people have some lingering tenderness with kneeling into adulthood.
The goal is not to win against the knee. It is to teach your child how to manage it: listen to pain signals, recover well, and keep moving in ways that do not aggravate the growth plate.
Return to sports
Parents often ask, “Do we have to stop sports?” Usually, no. But we do want a smart plan.
Increase activity when:
- They can walk and climb stairs without limping
- Pain is mild and does not worsen during practice
- Pain does not cause them to change their form (no favoring one leg)
- They can do a gentle squat and small hop without sharp pain at the bump
- Symptoms are not significantly worse the next morning
If your child plays on multiple teams, this is the moment to be extra honest about total weekly load. Many knees do fine with one season at a time and struggle with overlapping leagues plus private training.
Quick parent pep talk
If your child is tough and competitive, they may minimize pain. If your child is sensitive or anxious, they may fear something is seriously wrong. Both responses are normal. Your job is to keep the message calm and steady: “This is common, it is treatable, and we will adjust things so your knee can keep up with you.”
And if you needed permission to say no to that extra tournament weekend, consider this it.


